#TCTAP 2024 #PCI live case #Dou Kefei,MD &Yin Dong,MD Fuwai hospital

TCTAP, as a summit in the Asia-Pacific region, enjoys an outstanding reputation in the field of cardiovascular intervention. By gathering global wisdom, promoting academic exchanges, and driving technological innovation, it has made important contributions to the development of cardiovascular. With the continuous advancement of technology and the deepening development of the medical field, it is believed that TCTAP will continue to play a leading role in the field of cardiovascular in the Asia-Pacific region and make greater contributions to the cause of human health.
On April 26, 2024, during the 29th TCTAP conference in South Korea, Professor Ke-Fei Dou and Professor Dong Yin's team from Fuwai Hospital, Chinese Academy of Medical Sciences, were invited to live broadcast a high-difficulty percutaneous coronary intervention (PCI) for chronic total occlusion (CTO) of the right coronary artery (RCA) to cardiovascular doctors worldwide. The patient had a long RCA CTO lesion with tortuosity, calcification, unclear entry, and was a previously failed case, with a J-CTO score of 4 points. Professor Dou's team successfully opened the lesion for the patient using a Hybrid strategy of antegrade wire escalation (AWE) and timely controlled antegrade-retrograde subintimal tracking (Reverse CART, hereafter referred to as R-CART). Experts at the conference contributed their wisdom and experience, while the surgical team spared no effort, presenting an extraordinarily brilliant surgical demonstration.
.

The patient is a 51-year-old male with a history of hyperlipidemia. His medical history is complex. In February 2014, he was diagnosed with ST-segment elevation myocardial infarction (STEMI), for which he underwent percutaneous coronary intervention (PCI) with placement of two stents in the left main coronary artery-left anterior descending artery (LM-LAD), one stent in the left circumflex artery (LCX), and one stent in the intermediate branch. In December 2023, he was diagnosed with stable angina. Coronary angiography (CAG) on December 31st revealed chronic total occlusion (CTO) of the proximal right coronary artery (pRCA) and in-stent restenosis (ISR) in the LCX stent. Re-opening of the RCA CTO failed, and drug-coated balloon (DCB) treatment was performed on the LCX.
Echocardiography showed a left ventricular dimension of 51mm, an ejection fraction of 59%, and regional wall motion abnormalities. Coronary angiography results indicated that the LM-LAD, LCX, and first obtuse marginal branch (OM1) stents were patent, while the proximal-mid right coronary artery (p-mRCA) had a long CTO lesion.
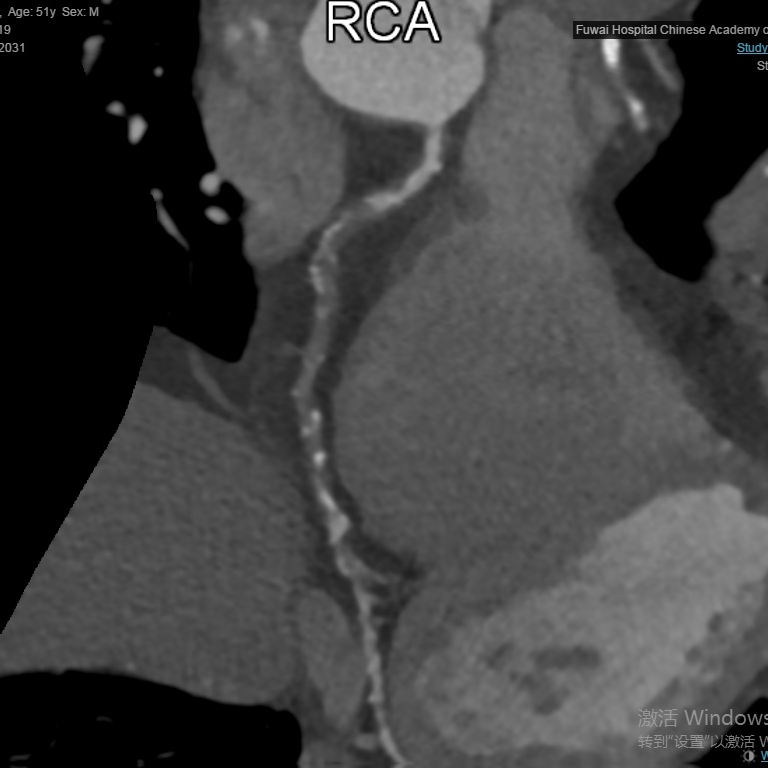
According to the right coronary artery (RCA) CTA imaging, the patient's chronic total occlusion (CTO) lesion appears to be long and accompanied by calcification. The patient's J-CTO score is 4 points.
Strategy:The aim of this surgery is to address the Right Coronary Artery (RCA) chronic total occlusion (CTO) lesion. The planned surgical strategy involves puncture under Intravascular Ultrasound (IVUS) guidance, followed by Antegrade Wire Escalation (AWE) technique. An alternative approach is to utilize Guidezilla assistance for retrograde operations, employing the Reverse Controlled Antegrade and Retrograde Subintimal Tracking (R-CART) technique.
Preoperative Considerations:
How to plan the strategy for RCA CTO PCI?
When and how to timely transition to the Hybrid CTO PCI strategy?
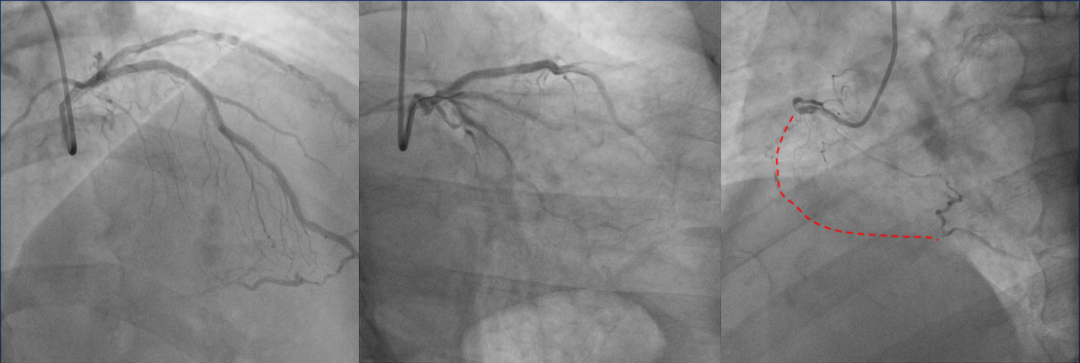
Preoperative coronary angiography revealed a long chronic total occlusion (CTO) lesion in the proximal-mid right coronary artery (p-mRCA) (Animation 1). Initially, an attempt was made to antegradely open the lesion, using intravascular ultrasound (IVUS) to locate the entry point of the occluded segment. However, the UB3 guidewire assisted by KDLC (dual-lumen microcatheter) failed to pass through the lesion (Animation 2). Subsequent IVUS imaging showed the guidewire positioned correctly at the entrance of the CTO, prompting a switch to Corsair microcatheter and Pilot200 guidewire for another antegrade attempt. Due to the length of the CTO lesion, as well as its tortuosity and calcification, the guidewire could not pass through the occluded segment, leading to the decision to proceed with retrograde intervention. With assistance from the APT 1.7F 150cm microcatheter, the retrograde SUOH 03 guidewire (which has a finer distal end compared to the Sion series, providing better flexibility and torque control, suitable for passing through curved side branch vessels) successfully entered the distal RCA through an interventional collateral channel (Animation 3). However, subsequent attempts using Pilot200 and UB3 guidewires for retrograde passage through the CTO lesion were unsuccessful (Animation 4). Recognizing the challenge posed by the calcified lesion at the angulated corner, and after consultation with on-site experts, the decision was made to initiate the retrograde Reverse Controlled Antegrade and Retrograde Tracking (R-CART) technique. Although both antegrade and retrograde guidewires were within the structure, they were too far apart to ensure successful R-CART. Through the use of dual-lumen microcatheter antegradely and constant adjustment of the position of the second guidewire, both antegrade and retrograde guidewires were brought extremely close together. Simultaneously, the use of a relatively stiff CP guidewire antegradely facilitated penetration of the calcified portion (Animation 5). The Pilot200 guidewire was then switched again to adjust the direction, bringing the antegrade and retrograde guidewires into basic alignment (Animation 6). At this point, R-CART was initiated, with full antegrade dilation using a 2.5mm balloon, successful puncture of the retrograde guidewire, and antegrade introduction of Guidezilla to assist the retrograde guidewire entry, followed by a reverse rendezvous to externalize (Animation 7). IVUS confirmed that the guidewires were within the true lumen throughout the procedure, and three stents were successfully implanted in the RCA, resulting in restored blood flow (Animation 8). Postoperatively, the patient's hemodynamics remained stable, and there was a significant improvement in cardiac function.
Animation1(L);Animation2(R)

Animation3(L);Animation4(R)
Animation5(L);Animation6(R)

Animation7(L);Animation8(R)
Regarding when and how to timely switch to a Hybrid CTO PCI strategy, Professor Ke-Fei Dou remarked: "For clinically complex lesions, we need to refine our diagnosis and treatment strategies. It's crucial to develop a Hybrid strategy combining antegrade and retrograde approaches tailored to the specific conditions of each patient to ensure the smooth progression of CTO PCI technology. Under bilateral angiography, we assess whether the proximal cap is clear, whether distal opacification is good, and whether the length of the occluded segment is <20mm. If all criteria are met, we proceed with antegrade wire techniques. If unsuccessful, we promptly switch to a retrograde strategy."
The Reverse Controlled Antegrade and Retrograde Tracking (R-CART) technique is a coronary intervention technique developed based on retrograde wire techniques. Compared to traditional CART techniques, R-CART offers the advantages of being relatively safe and simple to operate, thus garnering widespread attention and application among coronary interventionists. Several points to note during operation include: 1. Bringing the antegrade and retrograde guidewires as close as possible. Only when both are sufficiently close can the success rate of R-CART be higher. 2. Using a dual-lumen microcatheter antegrade can help bring the antegrade guidewire as close as possible to the retrograde guidewire. 3. Guidezilla can assist the retrograde guidewire in smoothly entering the antegrade guiding catheter. 4. Reverse Rendervouz technology can overcome weaknesses such as difficulty pushing retrograde microcatheters and RG3 pulling the heart.
发表留言
暂无留言
输入您的留言参与专家互动